
Credit: Nahrizul Kadri
We’re exploring an emerging question at the intersection of clinical care, software, and artificial intelligence (AI):
How should AI be used in a clinic to support care in a way that best protects patient privacy?
This work is still very early, and that’s intentional. We don’t have final answers yet, but we do have clear priorities: protecting patient privacy, maintaining safety, and ensuring that any use of AI remains fully under clinical and organizational control.
In healthcare, that means being deliberate about how patient data is used, while staying open to innovation and new tools that could meaningfully impact care.
This is an area where progress is important, and where moving too slowly or too cautiously could also limit potential benefits. At the same time, any advancement needs to be approached carefully, with appropriate safeguards in place.
There are still many open questions, and that’s exactly why we’re taking an iterative approach — starting small, learning as we go, focusing on how AI can contribute to clinical work in a responsible, controlled, and well-governed way.
WHY EXPLORE AI AT ALL?
Large amounts of patient information are already managed across primary care teams and clinical systems every day — reviewing charts, identifying relevant history, tracking preventative care needs, and helping patients navigate complex healthcare information.
Some of this work is clinical and decision-based, while some of it is administrative, repetitive, or difficult to manage with traditional tools alone.
The goal of exploring AI in this context is not to replace clinical judgment or automate care decisions. Instead, the aim is to understand how AI may support specific categories of healthcare work where existing processes can be time-intensive, hard to scale, and challenging to execute consistently across systems and workflows.
In practical terms, this may include:
Information retrieval and chart navigation tasks: Using an AI-assisted tool inside the EMR that helps clinicians more quickly surface relevant information from large patient charts for review, rather than manually searching through records.
Population-level care and preventive workflows: For example, identifying groups of patients who may benefit from specific care pathways (e.g., congestive heart failure or COPD programs) or surfacing preventative care gaps across a patient panel.
Low-risk administrative and documentation support: Such as organizing and classifying documents, or helping streamline required tasks by generating first drafts of documentation and summaries.
Complex, large-scale record and triage workflows: AI may also assist with preventive care triaging and large-scale record review, helping care teams complete workflows that are technically possible today but difficult to perform efficiently and consistently across large patient populations.
Throughout all of this, clinicians and care teams remain fully responsible for reviewing information, exercising judgment, and making decisions about patient care.
As with work produced by a medical learner or other clinical support role, AI-generated outputs would be thoroughly reviewed and validated by clinicians in the same way.
WHY “LOCAL AI”?

Credit: Maksym Kaharlytskyi
AI in healthcare naturally raises important questions around privacy, and it should. Patient data is highly sensitive, and how it’s handled matters.
Privacy is the starting point for this work, with a key focus on where and how data is processed.
In many current healthcare AI tools, such as AI scribes, patient information is sent to external, cloud-based systems for processing. Our first use of AI was in this space, and more about our AI and software work can be read here.
These tools can meaningfully reduce administrative burden and support clinical workflows, and we continue to use them where appropriate.
For this exploration, however, we are intentionally focused on a different approach — local AI systems that run within clinic-controlled infrastructure.
That means:
Patient data stays inside the clinic environment
Information is not sent to public AI platforms
Data is not used to train third-party models
Access is limited, governed, and auditable
Any use is tied to specific, appropriate clinical purposes
When AI is used in healthcare, it should be designed from the ground up to respect the sensitivity of patient information.
WHAT THIS LOOKS LIKE IN PRACTICE
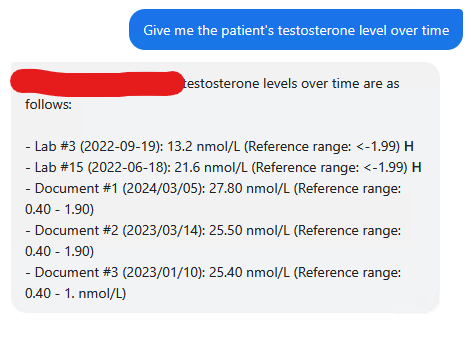
Example of AI-assisted chart review: The AI retrieves and organizes the patient's testosterone results over time, including relevant lab values and dates, for the clinician to review.
This work is still in its early stages.
We’re exploring how AI capabilities could be built directly into our open-source electronic medical record (EMR), where clinicians could interact with tools in a controlled, internal environment.
The funding behind this work — a combination of primary care funding and seed funding — is being directed toward exploring how local AI might be safely integrated into clinical workflows.
The goal is to use focused, intentional investment to explore ideas that could have an exponential long-term impact.
Some early directions being explored include:
Helping clinicians review large charts more efficiently — for example, surfacing relevant history when a new patient is seen after hours, so clinicians can quickly orient themselves to key clinical information. In practice, a clinician seeing an unfamiliar patient after hours for an asthma-related concern could ask the AI to summarize the patient's history of prescribed asthma medications and the documented response to each one, rather than manually reviewing several years of records.
Supporting privacy and quality processes — such as assisting staff in reviewing transferred records, where identifying missing or misfiled information can require careful review. Closing the loop on missing medical information is an important part of care delivery at Magenta Health, and you can read more about that work here.
Improving preventative care workflows — helping identify patients who may benefit from follow-up care based on existing criteria, such as screening eligibility or care gaps. For example, highlighting when a patient is due for a mammogram, or when family history suggests earlier screening may be appropriate.
Improving how information is communicated — for example, translating complex clinician-centred documentation into clearer, more accessible language for patients.
Supporting structured summaries of existing patient information — generating clear overviews of medical history to assist preventive care conversations or annual health reviews, where large amounts of patient information need to be reviewed in a structured format.
Importantly, none of this is about introducing new data collection. Instead, it focuses on helping clinicians and care teams better access, interpret, and act on information that already exists in the record.
EARLY-STAGE EXPLORATION THROUGH <BETTER/CARE>
At this stage, local AI isn’t a finished product or deployed system. It’s an early exploration, intentionally small in scope, focused on learning, and guided by a central question:
If AI is used in healthcare workflows, how can it strengthen privacy, support clinicians, and improve care delivery?
This work sits within our broader <Better Care/> campaign — an ongoing effort to improve the open-source EMR system that powers nearly every part of primary care in our clinics, and in healthcare settings across Canada.
If you’d like to learn more about the work behind <Better Care/> or how you can contribute to these improvements, you can find more information here.
There are many possible applications of AI in healthcare. Some may prove valuable, some may not, and some may not be appropriate at all. That uncertainty is exactly why careful exploration matters.
For us, the most exciting part is the possibility that AI can help healthcare teams do the work they already do more consistently, efficiently, and at a greater scale. If that proves possible, it could mean better support for clinicians, more reliable systems, and ultimately better care for more patients.
But first, it has to earn that role. For now, we’re focused on moving carefully, learning as we go, and doing it right.